Case Presentation of Imperforate Hymen and the Utilization of Pelvic POCUS in the Emergency Department
The Case
12-year-old female previously well presented to the ED for abdominal pain that had been ongoing for the past 7 days. Pain started as crampy and periumbilical. She was initially evaluated by pediatrician a few days prior to this who palpated a left lower quadrant mass and thought it to be increased stool burden. The patient was started on MiraLax. Over the next 2 days her pain moved down to her vaginal area and she noticed that there was something protruding from her vagina. She also felt that she had some pressure with urination and that sitting made her pain worse. She noted that she has never had a period and is not sexually active.
The patient denied any other systemic symptoms including fever, chills, headache, lightheadedness, chest pain, shortness of breath, cough, nausea, focal neurologic deficits. She is up-to-date on immunizations and denied any sick contacts.
Physical exam showed suprapubic fullness and distention with bulging blue-tinged mass obstructing the vaginal introitus. The patient was very uncomfortable-appearing and had difficulty lying flat on her back due to discomfort. Remainder of abdominal exam was soft and non-tender.
Given physical exam findings there was concern for imperforate hymen or other GU pathology decreasing communication between the uterus and external vaginal surface. Point-of-care ultrasound was performed at this point and confirmed backup of blood in vaginal vault (hematocolpos) and a small amount of fluid in the uterus (hematometra), concerning for imperforate hymen.

A radiology-performed ultrasound was ordered. In the meantime, acute care surgery was consulted. The patient ultimately went to operating room for hymenectomy with drainage of approximately 400 mL retained blood in vaginal canal.


Imperforate Hymen
Brief Embryology review
The female reproductive system begins to form at approximately the third week gestation but remains undifferentiated until approximately the fifth or sixth week of fetal life. At this point there are the mesonephric and paramesonephric systems. Based upon the anti-mullerian hormone and SRY gene in females, the mesonephric ducts begin to regress and the paramesonephric ducts continue on to further differentiation. The paramesonephric duct becomes the uterus, fallopian tubes, cervix, and upper third of vagina. The remainder of the vagina is created from the sinovaginal bulbs which originate from the urogenital sinus and eventually fuses with the uterovaginal canal formed from the paramesonephric ducts. There is degeneration of the central canal of this plate which forms the vaginal canal. During this process there is a hymenal membrane that separates the vaginal lumen from the urogenital sinus. The hymen usually ruptures before birth due to degeneration, but this can persist as a thin mucous membrane around the vaginal introitus [1,2].

Uterine/vaginal formation [2]
What is the common presentation and diagnosis of imperforate hymen?
Symptoms are dependent upon whether there is a complete or partial obstruction. It may be diagnosed in neonates as a bulging sac from the introitus due to muco-colpos from vaginal secretions. This typically gets resorbed, and patient will be asymptomatic until menarche. If the hymen remains imperforate, the vaginal outflow tract is obstructed, resulting in menstrual blood to accumulate in the vagina (hematocolpos) and/or uterus (hematometra). Consequently, patients will often present with primary amenorrhea. They will commonly develop pain in the lower abdominal quadrants following a cyclic nature corresponding to menstrual cycles. If hematocolpos occurs, patients may present with a bluish bulging obstruction in the vagina. Other common presenting symptoms include abdominal distention, urinary retention, dysuria, urinary frequency, frequent UTIs, and back pain. There is also the possibility of complications including infection of the retained blood products in the vagina. [3-4]
Indications for diagnostic Imaging
Diagnosis can be made on physical exam in many cases. If the classic suprapubic distention with hemato-colpos is seen on pelvic exam, no further imaging is required. Transabdominal ultrasound is the first line of imaging to ensure there is not distal vaginal abnormality. If the distal vaginal is patent and further detail is needed, then a transvaginal ultrasound can be performed. MRI is usually the last line of imaging and is indicated when the clinical picture is uncertain and/or if there is suspicion for further gynecologic abnormalities, most notably vaginal atresia, as this often requires more complicated surgical management and planning [5]
Technique for transabdominal pelvic ultrasound [6-7]
Patient positioning: Place patient in supine position with knees flexed if possible
Probe Selection: Low frequency curvilinear probe works best as this provides the depth needed to assess the uterus and areas deep to the GU tract.
Technique: Expose lower abdomen and pelvic area. Obtain a midline sagittal view and fan the probe left and right to assess the lateral aspects of the pelvis. Attempt to include the ovaries if possible. Then rotate the probe 90 degrees to obtain a transverse view, and fan the probe superiorly and inferiorly to image the entire pelvis. For both views, ensure there is adequate depth to see behind the bladder and uterus to assess for free fluid.
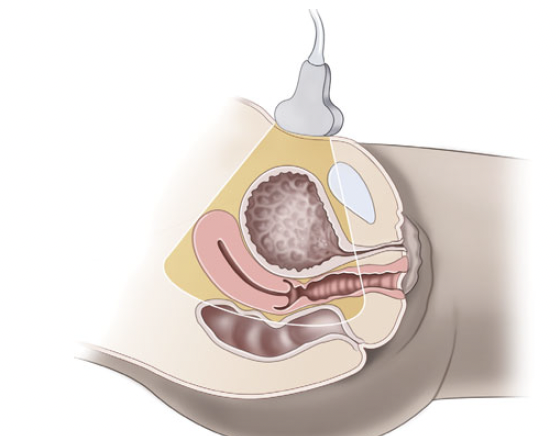
Pelvic anatomy & probe placement [7]]

Sagittal view
Transverse pelvis [7]
Troubleshooting: If there is difficulty with visualization attempt to hydrate patient to fill bladder. This creates an acoustic window to improve penetration of ultrasound waves leading to improved visualization of deeper structures. If still unable to visualize structures then consider transvaginal ultrasound. For any fluid collections or masses place color-flow or Doppler to assess for vascularity.
Findings suggestive of imperforate hymen: dilated and fluid-filled vagina (hematocolpos) +/- uterus (hematometra) - both seen in this patient’s case. Note that this fluid is well-circumscribed, unlike free fluid which usually has sharper/irregular edges.

Differential Diagnosis
Agenesis of distal vagina: Another presentation of amenorrhea. Ultrasound can be performed and will find dilation of proximal vagina and possibly uterus with absence of distal vagina [8]

Agenesis of distal vagina [8]
Urinary tract obstruction: Ultrasound will show large dilation of the bladder with normal-appearing uterus and vagina. An ultrasound should also be performed of the bilateral kidneys to assess for hydronephrosis. There may also be a visualized mass in the bladder which could explain bladder obstruction.

Distended bladder with hydronephrosis [9]
Urinary tract infection: May cause suprapubic tenderness but will likely have normal ultrasound findings [9]
Pelvic inflammatory disease/tubo-ovarian abscess: Best evaluated using transvaginal ultrasound. PID will best be visualized using color Doppler which will possibly show a fluid-filled slightly distended endocervical canal with hyperemia. It is also important to visualize the fallopian tubes as well as ovaries to assess for nephritis and pyosalpinx/tubo-ovarian abscess. Pyosalpinx will show dilation of the fallopian tubes with hyperechoic fluid and hyperemia noted on color Doppler [10]

Cervicitis [10]

Pyosalpinx [10]
Intra-abdominal pathology: can assess for bowel obstruction, appendicitis, or significant stool burden. Often better assessed for using CT imaging.
Management
Management of imperforate hymen is dependent upon age and stage of development of patient. When imperforate hymen is suspected in pre-pubertal stage without hemato-colpos, then intervention is often delayed until the beginning of puberty. In these early stages it is difficult to differentiate between imperforate hymen and vaginal atresia so management should be delayed until the gynecologist can confirm the presence of a uterus and patent vagina. At this point, surgical hymenectomy is warranted to decompress uterus and vagina assuming no other abnormalities exist. [5]
Take Home Points:
Suspect imperforate hymen as a cause of abdominal pain and amenorrhea.
POCUS is a quick and effective way to confirm diagnosis if physical exam is not conclusive or further detail is requested by surgical team.
Ensure there are no other gynecologic abnormalities prior to definitive management.
When performing pelvic POCUS ensure adequate depth is used to assess for free fluid and pelvis is fully assessed in both sagittal and transverse views.
POST BY: DR. CONNOR PARSELL (PGY2)
FACULTY EDITING BY: DR. LAUREN MCCAFFERTY (ULTRASOUND FACULTY)
References
Moncada-Madrazo M, Rodríguez Valero C. Embryology, Uterus. [Updated 2021 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK547748/
Laufer MR. Congenital anomalies of the hymen and vagina. In: UpToDate, Barbieri RL, Levine D, Chakrabarti A (Ed). UpToDate; 2022. Accessed 4 Feb 2022. https://www.uptodate.com/contents/congenital-anomalies-of-the-hymen-and-vagina/
Lee K, Hong J, Jung H, Jeong H, Moon S, Park W, et al. Imperforate Hymen: A comprehensive systematic review. J Clin Med. 2019; 8(1), 56.
Lardenoije C, Aardenburg R, Mertens H. Imperforate hymen: a cause of abdominal pain in female adolescents. BMJ Case Rep. 2009;209:bcr0820080722
Oelschlager A, Anne-Marie E, Berger-Chen SW.. Management of Acute Obstructive Uterovaginal Anomalies. Obstetrics & Gynecology. 2019; 133(6).
Noble V, Nelson B. (2011). Abdominal aorta ultrasound. In Manual of Emergency and Critical Care Ultrasound (pp. 115-132). Cambridge: Cambridge University Press.
Ma OJ, Mateer JR, Reardon RF, & Joing S. (2014). Ma and Mateer's Emergency Ultrasound. New York, NY: McGraw-Hill Education.
Stec AA, Wang MH. Isolated distal vaginal agenesis masquerading as recurrent urinary infections in an adolescent female. J Pediat. 2011; 158(4), 684.
Halbgewachs C. Postobstructive diuresis: Pay close attention to urinary retention. Canadian Family Physician. 2015; 61(2), 137–142.
Revzin MV, Mathur M, Dave HB, Macer ML, Spektor M. Pelvic inflammatory disease: Multimodality imaging approach with clinical-pathologic correlation. RadioGraphics. 2016; 36(5), 1579–1596.